Problem Behavior at Home and in the Community: When Is It Most Likely To Occur? A Guide for Parents
March 01, 2005
Note to readers: In keeping with OAR’s interest to make research results understandable to the widest possible audience, we require each of our researchers to provide a Research Summary written in layman’s terms for the primary target audience, parents of children with autism, upon completion of their research. Below is a summary of research by Edward G. Carr, Ph.D., BCBA, FAAMR, who recently completed a study on problem behavior funded by OAR in 2004. A leading author and presenter on behavior issues, Carr’s findings detail ways to decrease problem behavior in individuals with autism by developing an effective method to assess the cause or causes of the behavior.
“I dread mealtimes,” Mrs. Johnson told us. “That’s when Timmy is most likely to explode. We’ve given up on trying to eat together as a family.” Mrs. Juarez said that, “If she and her husband don’t provide Ramon with attention whenever and wherever he wants it, they can count on him biting himself and hitting himself. They are physically and emotionally drained.” Mrs. Robinson told us that, “When Aisha was put on medication for her aggressive behavior, she thought that she could see the light at the end of the tunnel. Instead, the medication seemed to make Aisha irritable, constipated, and tired all the time. Her aggression actually got worse. We give up.”
Does any of this sound familiar to you? Many parents have experienced the sorts of situations just described so you are not alone. Each of these situations are referred to as “contexts” for problem behavior. Problem behavior, whether it is aggression, self-injury, tantrums, or some other form of disruptive behavior is very common in children with autism and can make family life pretty miserable. Furthermore, such behavior is the leading cause of institutionalization and reinstitutionalization, and is associated with rejection by peers as well as exclusion from neighborhood schools. In adulthood, problem behavior is a major reason why people with autism are unemployable. All of these issues add up to increased stress and poor quality of life for family members. So it is important to help families identify the “contexts” that set off problem behavior. This knowledge can then be used to help plan effective treatments.
Of course, the number of contexts that can set off problem behavior is potentially limitless. It would take forever to ask parents to identify each and every possible context that might be relevant to their particular child. We need an efficient way to narrow down the possibilities.
The purpose of our OAR-funded research project was to develop a user-friendly inventory that parents could fill out in order to zero in on those contexts relevant to their child, as a way of jumpstarting the process of building interventions based on accurate, useful information. We began to develop our inventory by reviewing all of the scientific literature to date that described the kinds of contexts that were most likely to set off problem behavior. We noticed that the contexts described seemed to fall into three categories: social, activities/routines, and biological. Social contexts involved aspects of the environment that were related to interactions among people; for example, “My child becomes frustrated when he or she has trouble communicating his/her needs.” Activities/routines involved common situations that occurred, often on a daily basis, as an integral part of family life; for example, “I sometimes have to interrupt my child when he/she is engaged in a preferred activity, such as playing outside, to ask him/her to come inside to eat or take a bath. This makes my child very angry.” Biological contexts referred to a child’s state of health or physiological condition; for example, “When my child is frightened or tired, he/she can become explosive.”
Once we compiled lists of context items from the scientific literature, we whittled the list down to the most frequently described items and defined each one of them with a concrete example. So, if the item was “shows problem behavior when a preferred activity ends,” we gave an example such as, “Your child is playing with his favorite videogame and you ask him to turn it off and get ready for bed.” We then created a scale that allowed parents to indicate how likely it was that a specific situation would set off problem behavior by choosing a number from 1 to 5 (1 = Not likely; 3 = Somewhat likely; 5 = Very likely; DK = Don’t know; NA = Not applicable to my child). Finally, we sent the preliminary inventory that we have just described to a large number of experts and family members asking them to provide us with feedback on the clarity of instructions we gave for completing the inventory, whether the inventory was easy to understand, and whether the inventory excluded some important contexts that ought to be listed. Based on this feedback, items were deleted, rewritten, or added as appropriate.
Once we completed the process just described, we were able to create an inventory that we named the Contextual Assessment Inventory (CAI). The CAI, as mentioned before, had three categories: social, activities/routines, and biological. Each category, in turn, was comprised of eight contextual items. For the social category, the context items were: (1) disagreement among family members, peers, or others; (2) recently disciplined; (3) being teased; (4) hurried or rushed; (5) not enough attention from others; (6) frustrated because of an inability to communicate personal needs; (7) denied access to desired items or activities; (8) bad day at school or other activity taking place outside of the home. For the activity/routines category, the context items were: (1) a preferred activity ends; (2) activities/routines are difficult, frustrating, disliked, or boring; (3) activity is too long; (4) activity is too noisy/crowded; (5) having to wait; (6) medical appointments; (7) changes in routines; (8) transitions between settings/activities. For the biological category, the context items were: (1) medication side effects; (2) illness/pain; (3) feeling tired; (4) feeling hungry/thirsty; (5) feeling hot/uncomfortable; (6) frightened; (7) sad/depressed; (8) sexual frustration. Mothers and fathers were asked to fill out the inventory for their children. Shortly, we will describe for you the results we got for the first 106 parents who completed the CAI. (Additional families are currently being asked to complete the CAI so that eventually, the number of parents will be substantially greater than this.) After a period of four to six weeks (on the average) had passed, we asked parents to complete the CAI again to check to see how stable the ratings were.
 Figures 1 (Social), 2 (Activities/Routines), and 3 (Biological) show the context factors that parents identified as most likely to set off their children’s problem behavior. If you review the data on Figure 1 (Social), you will see the context factors arranged from most nominated (according to mothers) as well as the ratings made by fathers. Please note that a “nomination” means that the mother or father felt that a particular context item was “very likely” (a 4 or 5 on the scale described previously) to set off problem behavior. So, in Figure 1, we see that almost 80 percent of the mothers said that when their child was denied access to something that he/she really wanted, the child was very likely to show problem behavior. About 55 percent of fathers nominated “denied access” as well. In general, mothers and fathers tended to agree with each other about which contexts set off problem behavior in their children, an occurrence scientists call “inter-rater reliability.” That is, the two evaluators (mother and father)
Figures 1 (Social), 2 (Activities/Routines), and 3 (Biological) show the context factors that parents identified as most likely to set off their children’s problem behavior. If you review the data on Figure 1 (Social), you will see the context factors arranged from most nominated (according to mothers) as well as the ratings made by fathers. Please note that a “nomination” means that the mother or father felt that a particular context item was “very likely” (a 4 or 5 on the scale described previously) to set off problem behavior. So, in Figure 1, we see that almost 80 percent of the mothers said that when their child was denied access to something that he/she really wanted, the child was very likely to show problem behavior. About 55 percent of fathers nominated “denied access” as well. In general, mothers and fathers tended to agree with each other about which contexts set off problem behavior in their children, an occurrence scientists call “inter-rater reliability.” That is, the two evaluators (mother and father) 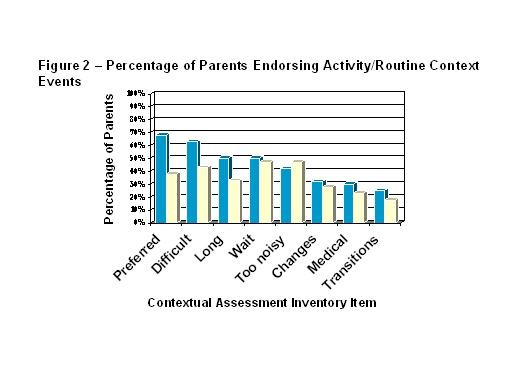 generally agreed with each other. This is a good thing because if a mother said certain contexts were very important and fathers disagreed, then we wouldn’t know in what area we had to intervene in order to solve the problem. It would also suggest that the mothers and fathers were confused about the nature and setting for the problem behavior. Fortunately, during our study, this was not the case. So, we can be pretty sure that the leading social contexts that set off problem behavior (Figure 1) were denied access, communication problems, and not enough attention; the leading activity/routine contexts (Figure 2) were preferred activity ends, difficult/disliked/boring tasks, activity too long, and having to wait; the leading biological contexts (Figure 3) were frightened, tired, hungry, and illness. Just because an activity was not nominated very often by a lot of parents (for example, “teasing” in Figure 1), it does not mean that the context was not important. It simply means that it was very important but only for a smaller number of children.
generally agreed with each other. This is a good thing because if a mother said certain contexts were very important and fathers disagreed, then we wouldn’t know in what area we had to intervene in order to solve the problem. It would also suggest that the mothers and fathers were confused about the nature and setting for the problem behavior. Fortunately, during our study, this was not the case. So, we can be pretty sure that the leading social contexts that set off problem behavior (Figure 1) were denied access, communication problems, and not enough attention; the leading activity/routine contexts (Figure 2) were preferred activity ends, difficult/disliked/boring tasks, activity too long, and having to wait; the leading biological contexts (Figure 3) were frightened, tired, hungry, and illness. Just because an activity was not nominated very often by a lot of parents (for example, “teasing” in Figure 1), it does not mean that the context was not important. It simply means that it was very important but only for a smaller number of children.
 It is worthy to note that we also asked parents to complete the CAI a second time, four to six weeks after they first completed it. When we compared what parents said the first time with what they said the second time, we found that the results were extremely similar, an occurrence scientists call “test-retest reliability.” It is highly favorable that test-retest reliability was so high because it means that the results are stable. If they were not, then we could not be sure that the CAI provides consistent (trustworthy) ratings and that would make it impossible to track problem behavior over time in a meaningful way that would help treatment planning and evaluation later.
It is worthy to note that we also asked parents to complete the CAI a second time, four to six weeks after they first completed it. When we compared what parents said the first time with what they said the second time, we found that the results were extremely similar, an occurrence scientists call “test-retest reliability.” It is highly favorable that test-retest reliability was so high because it means that the results are stable. If they were not, then we could not be sure that the CAI provides consistent (trustworthy) ratings and that would make it impossible to track problem behavior over time in a meaningful way that would help treatment planning and evaluation later.
We followed up with a number of families to see whether some context items that they nominated as being “very likely” to set off problem behavior actually did so in real-life settings. For example, if a mother said that “having to wait” was a context that set her child off, we asked the mother to give us an example of what she meant. If the mother said, “he hates waiting in line at the supermarket,” we went with her to the supermarket (with her permission) to observe whether indeed her child showed problem behavior in this situation. We did the same thing for some contexts that parents indicated were “very unlikely” to set off problem behavior. So far, we have done these “direct observations” with 14 families; more are in process. We found that, in every instance, when a mother, for example, said that the CAI item was “very likely” to set off problem behavior, it did. When a mother said it was “very unlikely” to do so, it did not. Scientists call this characteristic “validity.” It is again favorable that the CAI shows a high rate of validity. If it did not, that would mean that the CAI ratings did not measure what they were supposed to measure, namely, the contexts that actually set off problem behavior in real-life situations. The high validity of the CAI means that it can be used as a tool to provide accurate information about problem behavior and the contexts most closely associated with it, a great aid in treatment planning.
Finally, parents also told us that the CAI was: (1) comprehensive, that is, it appeared to include all the contexts that they could think of as being relevant to their child’s problem behavior; (2) comprehensible, that is, it was easy to understand and use, and (3) efficient, that is, it only took them about 21 minutes, on average, to complete.
The CAI appears to be a very useful assessment tool that parents can use to identify the contexts that are most likely to set off their child’s problem behavior at home and in the community. The CAI has good inter-rater and test-retest reliability. It appears to be valid, comprehensive, comprehensible, and efficient. Therefore, we should be able to use it to help accomplish the most important goal of all, namely, to design interventions that decrease problem behavior at home and in the community, thereby greatly contributing to family quality of life.
In fact, we have now developed a multi-component treatment approach, based on the CAI. The approach involves teaching parents how to avoid (where appropriate) those contexts that set off problem behavior, how to redesign the contexts to minimize problem behavior, and how to teach the child certain coping skills that make problem behavior unnecessary. Thus far, we have piloted our CAI-based treatment protocol with several families and have found that (1) we could dramatically reduce and, usually, eliminate problem behavior; (2) dramatically increase the degree to which families were able to participate successfully in a variety of home and community activities together; (3) increase the degree to which parents felt they were now in control; (4) decrease the level of stress that parents reported. Given these encouraging results, we are attempting to secure funds from either foundation or government sources so that the full benefits of our assessment/treatment strategies can be extended to help families who need such support now.
Inclusive Summer Ideas for Your Autistic Child
Summer gives you a chance to slow down and discover new rhythms with your autistic child. The longer days might...
Press Release: OAR Awards 10 Graduate Research Grants in 2025
ARLINGTON, VA, July 9, 2025 – The Organization for Autism Research (OAR) is delighted to announce the recipients of its...
Meet RUN FOR AUTISM Ambassador Beth
When Beth Caruso sought out her first marathon, she looked for a race that was, among other things, approachable. The...